Hoo boy: there is a lot to unpack today. Let’s get started.
Inflection Point
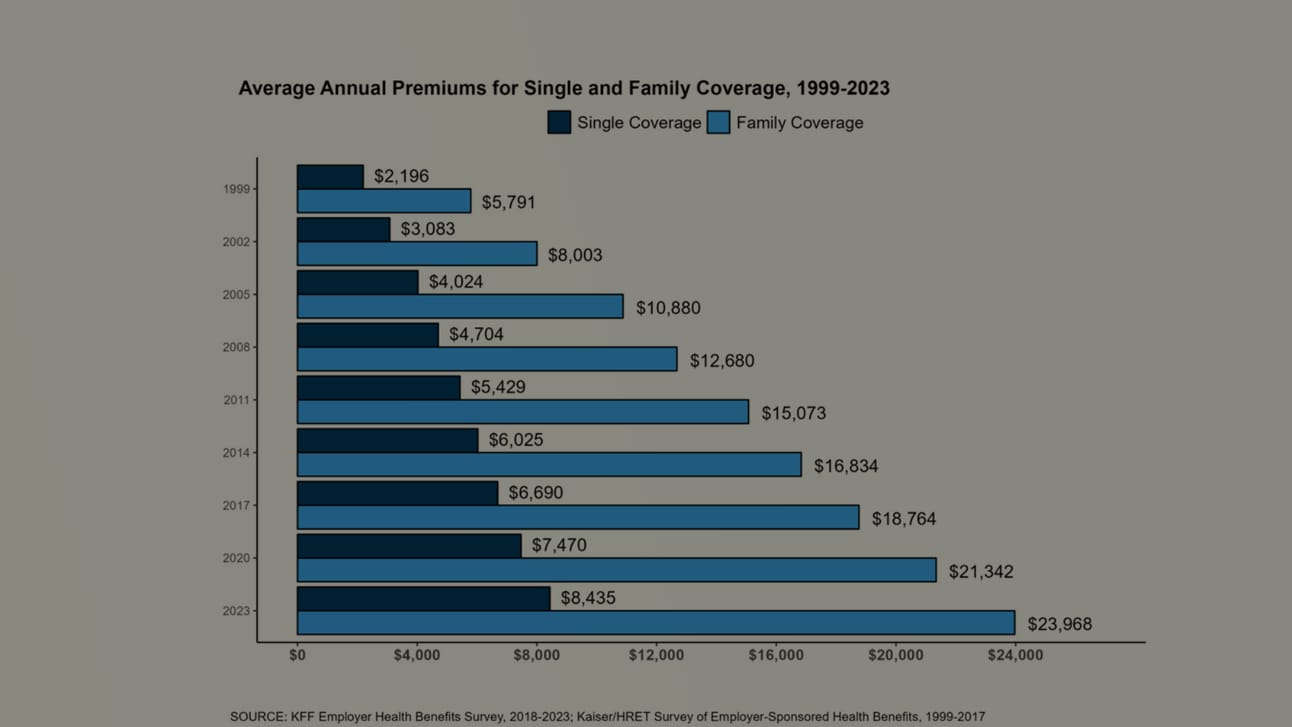
There may be no single document that is more useful for understanding where the U.S. health care system is (and how it got here) than the annual Kaiser Family Foundation Employer Health Benefits Survey, which gives an incredibly granular snapshot of what commercial insurance costs nowadays.
On that fundamental question — what does commercial insurance cost nowadays? — the answer is “a lot.” The answer is “a lot” every year, but — somehow — things keep getting worse. Premiums for the average family are now up around $24,000, up around 7%. Consumers themselves are on the hook for more than $6,500 of that.
So that drove the headlines.
A couple of additional notes:
First, it shouldn’t escape anyone’s notice that employers are doing worse (it’s a growing crisis for corporate America) and employees doing worse (a growing crisis in general). Pharmacists are pretty mad about reimbursement. Doctors are pretty mad about prior authorizations. And yet: UnitedHealth Group recorded record profits last quarter.
I’m not so mathematically challenged that I think that premiums are rising because health insurer profits continue to grow. I just worry that, maybe, the insurance industry doesn’t have enough skin in the game to really take the problem seriously.
Second — and this probably counts as good news, sort of — it seems like cost-sharing has hit kind of a ceiling. Deductibles are basically flat. I mean, they’re ridiculously high by any reasonable standard, but they’re not growing. And the trend of specialty drug tiers, which is basically a way to force additional cost-sharing, also seems to have stalled.
That doesn’t mean that things won’t get worse in the future. This is America. Coverage can always get worse in the future. But it means that, for a brief moment, those malign forces are taking a breather.
The Arc
It didn’t get much notice, but this AIR340B report on charity care by 340B hospitals really distills down the 340B debate: hospitals are seeing ever-larger revenues driven by the 340B drug discount program yet — at the same time — appear to be cutting charity care.
For the uninitiated, certain hospitals get massively discounted drugs under the 340B program. Rather than giving those cheap drugs to poor Americans directly, hospitals provide the medicines to fully insured patients, get reimbursed at the full rate, and pocket the difference between the 340B price and the reimbursed price.
So what are hospitals doing with all that extra money? The AIR340B report, driven by an analysis of federally reported data by Avalere, suggests that it’s not going to charity care, which fell to 2.5% of operating costs.
Hospitals generally claim that attacks on charity care lack a lot of context, but — on the flip side — hospitals aren’t exactly pushing for more transparency.
Quick Turns
- I’m not watching the Senate HELP hearing with would-be NIH chief Monica Bertagnolli — it’s going on as we speak — but I assume we’ll get some march-in questions. More tomorrow, probably.
- Cost-effectiveness assessments really need to have a better view of drug prices over the lifetime of a drug to be accurate. That’s why this Health Affairs Forefront piece from Tufts and NPC researchers, which makes the point that the IRA should be factored into value assessments, is so important. And it’s a reason to celebrate the fact that ICER is exploring the topic, too.
- When both the drug industry and UCSD’s Inma Hernandez agree on a policy solution, you can rest assured that it’s the right thing to do. So … Hernandez is out with a new paper that makes a compelling argument for Medicare coverage of obesity meds.
- I’m not sure that this Boston Globe profile of the Incubate coalition’s efforts to reform the IRA really gets deep enough into the details (I’m curious about the legislative state of play). But it’s worth noting that the group has basically accepted that price controls are a legitimate government effort. It’s only the 9-vs-13 thing that they’re opposed to.
- If you’ve lost track of all of the PBM-related legislation, the folks at McDermott+Consulting have you covered with this nice clip-n-save resource that summarizes all of the pending efforts.
- Oh, yeah: more obesity-drug stuff: If you’re looking for stories on second-order effects, here’s a piece on how more revenue for obesity-drug makers means more money for their charitable efforts (WSJ). And here’s Bloomberg’s entry in the ever-larger category of Overheated Coverage of How Obesity Meds Will Change Everything.
- But if you read just one obesity story today, please make it Damian Garde’s piece in STAT, which is helpfully headlined “The Ozempic panic: Why a market frenzy over new weight loss drugs defies logic.” It’s classic Garde. My favorite line? “Those concerns don’t seem to be resonating on Wall Street, a crowded theater in which about half the patrons are yelling ‘fire’ at any given moment.”

